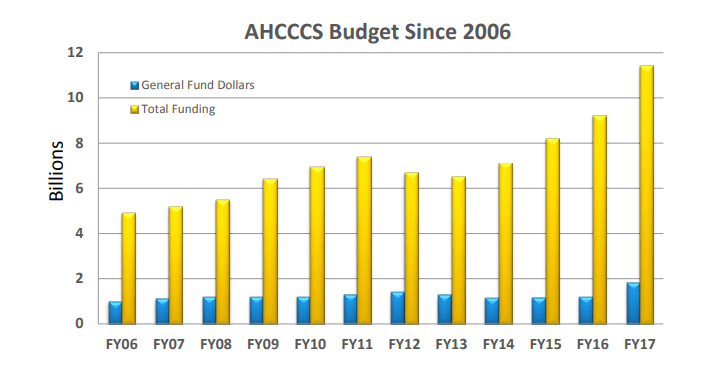
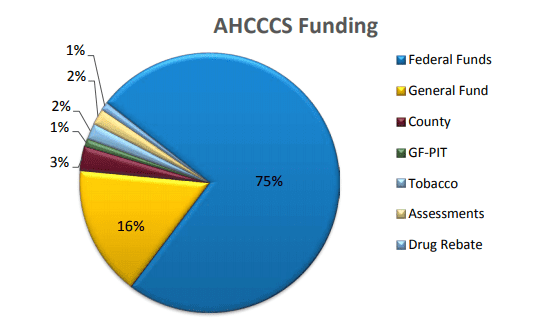
Everything costs money. Getting pregnant women dental coverage under AHCCCS is going to cost money to keep it going. Under the proposed bill SB1088, it could cost about $1.18 million to get it started [1]. I discussed in a previous blog about how Medicaid funding gets distributed and how oral health care is the smallest slice of the pie. You might remember that most of Arizona’s Medicaid funding comes from the federal government.
There are federal initiatives under the Affordable Care Act (ACA) that have recognized the importance of focusing funding preventative care (meaning healthcare that keeps people from getting sick or ending up in the hospital) and on improving the quality of care in order to actually save money and decrease the overall amount spent on health care. The United States spends more money on health care than any other developed nation, yet has some the worst health outcomes, especially when it comes to maternal and infant health. With the ACA comes a shift in thinking that is a benefit to what I want to see accomplished as far as getting dental coverage.
Dental care is a preventative service that has been shown to improve oral health status and prevent periodontal disease [5]. If periodontal disease is prevented, hypothetically, we can decrease the risk of preterm birth and low birth weight. Preterm birth alone cost an estimated $26.2 billion each year in the United States [6]. That number is astronomical. Preterm babies, those born before 37 weeks, often must stay in the hospital longer and are at risk for having trouble with breathing and feeding, having developmental delays, and having other conditions that require on-going and expensive care [2]. While dental care won’t eliminate preterm birth, over time it may help bring it down.

Prevention to improve the oral health of women takes time and time is money. But there are so many things the US government has already started doing to decrease healthcare costs and improve health outcomes. For example, the Centers for Medicare & Medicaid Services (CMS) has created a medical home model called Comprehensive Primary Care Plus (CPC+) [3]. This innovative plan is designed to improve primary care services by changing how care is delivered. It provides money for creating partnerships between health care organizations to work together to create a more seamless experience, to reduce unnecessary spending on repeat testing, and improve access to and the quality of care [3]. This process can easily be applied to integrating dental providers with perinatal providers.
CMS has also developed and funded an initiative to improve prenatal care for women with Medicaid [4]. The program goal was to decrease preterm birth rates among the most high risk groups of women. Funding for this program is no longer available, but when it was active, participating states received financial support to incorporate enhanced prenatal care and education, support for psychosocial needs, and coordination of care between different health care services [4]. This is another model that could easily incorporate dental care for women of Arizona. The goal is the same – improving the health and knowledge of at-risk pregnant women to decrease preterm birth.
Preventative oral health care falls right into these federal initiatives and ongoing funding can come from the health care savings seen with preventing poor outcomes. So let’s just bite the bullet, cough up the doe, and get this initiative started.

Thank you for joining me on my blog journey!
References
1. Arizona State Legislature. (2019). 2019 Fifty-fourth legislature: First regular session. SB1088. Retrieved from https://apps.azleg.gov/BillStatus/BillOverview/71280
2. Centers for Disease Control and Prevention. (n.d.) Reproductive health: Preterm birth. Retrieved from https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pretermbirth.htm
3. Centers for Medicare & Medicaid Services. (2019a). Comprehensive primary care plus. Retrieved from https://innovation.cms.gov/initiatives/comprehensive-primary-care-plus/
4. Centers for Medicare & Medicaid Services. (2019b). Strong start for mothers and newborns initiative: Enhance prenatal care models. Retrieved from https://innovation.cms.gov/initiatives/Strong-Start-Strategy-2/
5. Ide, M., & Papapanou, P. N. (2013). Epidemiology of association between maternal periodontal disease and adverse pregnancy outcomes–systematic review. Journal of Periodontology, 84(4), 181-94. doi: 10.1902/jop.2013.134009
6. March of Dimes (2019). The impact of premature birth on society. Retrieved from https://www.marchofdimes.org/mission/the-economic-and-societal-costs.aspx